Good kitty or bad kitty?
After three years of amazing litter box use (she even went in the litter box to cough up hairballs), my cat Muffin looked me in the eye and pooped right on a rug outside of her litter box. At first I thought she was sick. But then she played and acted normal for the rest of the evening. When I woke up in the morning, I noticed she had peed all over the rug. This was such unusual behavior.
I searched the internet and found many theories of cat behavior. Maybe she didnt like the new litter, maybe her box was too dirty, maybe she was upset. I decided to buy her a totally new litter box and went back to her fav kitty litter. I bought a slightly smaller box than she was used to because the other one had to squeeze into the fake furniture housing that encased it and I didn’t clean it as thoroughly as I should because it was challenging to get in and out.
It seemed to work! Muffin was doing her business back in the box. After a week or so when I took the box out to clean it, I noticed urine all underneath it. UGH! she was peeing outside the box. Maybe this was behavioral after-all. Time to google cat therapists.
Let’s look at this from a just culture lens.
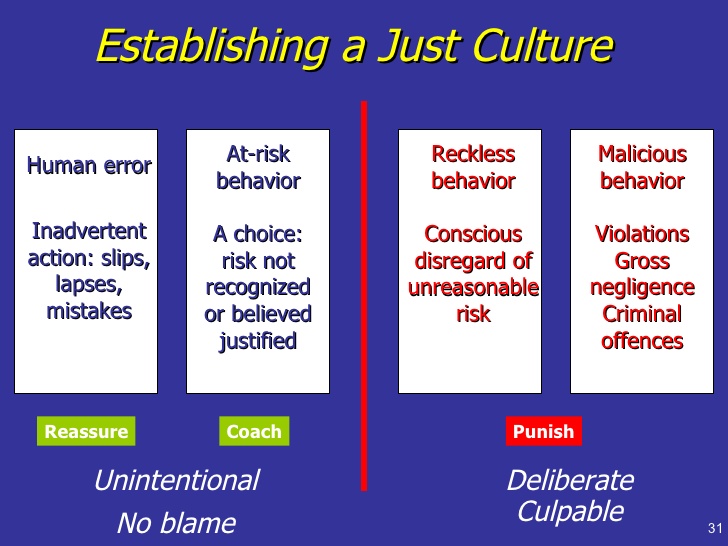
Initially I thought Muffin’s defiant voiding outside of her box was a protest…malicious behavior. Then after searching cat behavior, i thought maybe she was just being reckless. Then one day after cleaning all the urine under the litter box, i noticed that the side of the pan where she usually pees was pretty short. I flipped the pan around and put the taller side in that spot. Like magic problem solved! Muffin never meant to be malicious or reckless nor was she making a mistake! With a little redesign of her environment…problem solved! She just needed new better designed equipment.
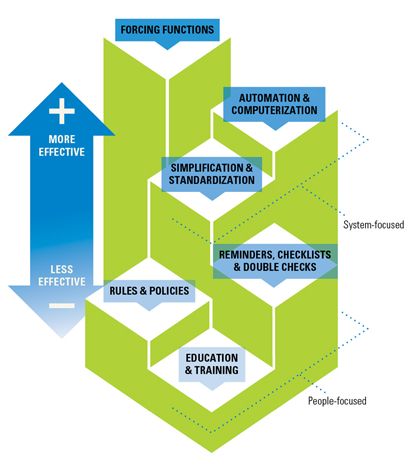
Do we support help our healthcare workers in redesigning their environment for safety or do we just accuse them of making errors and being reckless?