I have read much material lately about addressing the obesity epidemic and there are many commonalities in the latest theories.
1. Motivation- focusing on motivation as a strategy is not the best approach. Willpower has been dismissed by many as a poor approach to weight management
2. Behavior change- changing behaviors is not easy. Much of a person’s day consists of habitual activities resulting from cues from tv, peers, childhood… example wanting to eat popcorn while watching a movie, reaching for the salt before tasting food…
3. Environment changes-For obesity this holds the most promise. Its seen in weight watchers programs and Wansink’s book Slimdown by design. Change architecture and nudging can help make behavior change easier and lasting. This includes things like using smaller colorfull plates, moving healthy foods to a prominent kitchen spot and unhealthy foods to hidden cabinets. In some estimates people who follow certain environmental patterns are 18% thinner than those who do not.
What’s the correlation with patient safety?
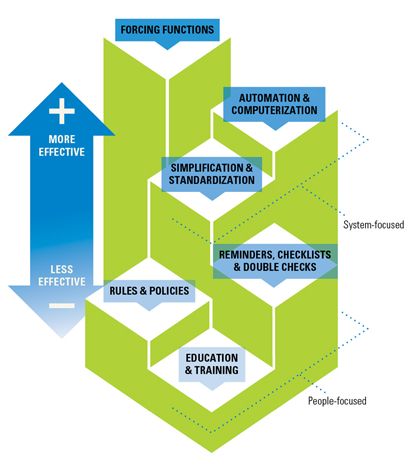
1. Motivation- focusing on motivation as a strategy is not the best approach. Motivating staff to be more vigilant? Teaching them? Telling them to Follow rules and policies? These have not been shown to increase safety measurably. In fact sometimes recognizing when to deviate from rules can add resilience
2. Behavior change- changing behaviors is not easy. Other articles on this cite describe many nursing behaviors as being based on tradition and automatic behavior. Often under stress people revert back to old knowledge. How many times has an initiative been rolled out only to see it vanished from practice within a year?
3. Environment changes- just as in obesity management here we might find the most bang for our buck so to speak. Make it easy for staff to do the right thing. Make it hard for staff to do the wrong thing. Create systems that nudge staff toward safe behaviors. Use change architecture to produce reliability
A healthier world depends on reducing obesity and unsafe patient care. Maybe the solutions to both are the same.
See Reference Page for some articles related to this page